
Vitamin D—how much is best? How much is toxic?

Clearing misconceptions about the many roles of vitamin D and the risk of toxic effects.
Vitamin D has numerous vital roles beyond bone health, especially for immune system function and the vital process of autophagy. Higher levels than those sufficient for calcium absorption are required. Typical reference ranges can be misleading.
Vitamin D is crucial for many non-skeletal functions including immune system regulation.
Numerous factors can interfere with vitamin D effectiveness, and there is significant individual variation in response to vitamin D.
Some individuals require very high doses for therapeutic effectiveness.
PTH (parathyroid hormone) levels in response to supplementation are a gauge of VDR (vitamin D receptor) response.
Toxicity is extremely rare; professionally managed, even ultra-high therapeutic doses have been given without toxicity.
It’s very common for providers untrained in functional medicine or clinical nutrition to question the recommendations for supplemental Vitamin D3 and the higher lab values that are in fact safe and effective in the case management of many chronic conditions. This brief review of the science is intended to inform and reassure both providers and patients.
Vitamin D deficiency is common
An informative paper written by perhaps the world’s leading authority on Vitamin D, Michael F. Holick, M.D., Ph.D., published in the New England Journal of Medicine, the author notes:
“Once foods were fortified with vitamin D and rickets appeared to have been conquered, many health care professionals thought the major health problems resulting from vitamin D deficiency had been resolved. However, rickets can be considered the tip of the vitamin D–deficiency iceberg. In fact, vitamin D deficiency remains common in children and adults.”
He points to crucial functions of vitamin D beyond skeletal health:
“The discovery that most tissues and cells in the body have a vitamin D receptor and that several possess the enzymatic machinery to convert the primary circulating form of vitamin D, 25-hydroxyvitamin D, to the active form, 1,25-dihydroxyvitamin D, has provided new insights into the function of this vitamin. Of great interest is the role it can play in decreasing the risk of many chronic illnesses, including common cancers, autoimmune diseases, infectious diseases, and cardiovascular disease.”
And notes that deficiency is very common:
“Much evidence suggests that the recommended adequate intakes are actually inadequate.”
Sunlight exposure is no guarantee of sufficiency:
“…even in the sunniest areas, vitamin D deficiency is common when most of the skin is shielded from the sun. In studies in Saudi Arabia, the United Arab Emirates, Australia, Turkey, India, and Lebanon, 30 to 50% of children and adults had 25-hydroxyvitamin D levels under 20 ng per milliliter.Also at risk were pregnant and lactating women who were thought to be immune to vitamin D deficiency since they took a daily prenatal multivitamin containing 400 IU of vitamin D (70% took a prenatal vitamin, 90% ate fish, and 93% drank approximately 2.3 glasses of milk per day)73% of the women and 80% of their infants were vitamin D–deficient (25-hydroxyvitamin D level, <20 ng per milliliter) at the time of birth…”
In a paper published in the Journal of Clinical Endocrinology & Metabolism, the authors state:
“More than half of North American women receiving therapy to treat or prevent osteoporosis have vitamin D inadequacy, underscoring the need for improved physician and public education regarding optimization of vitamin D status in this population.”
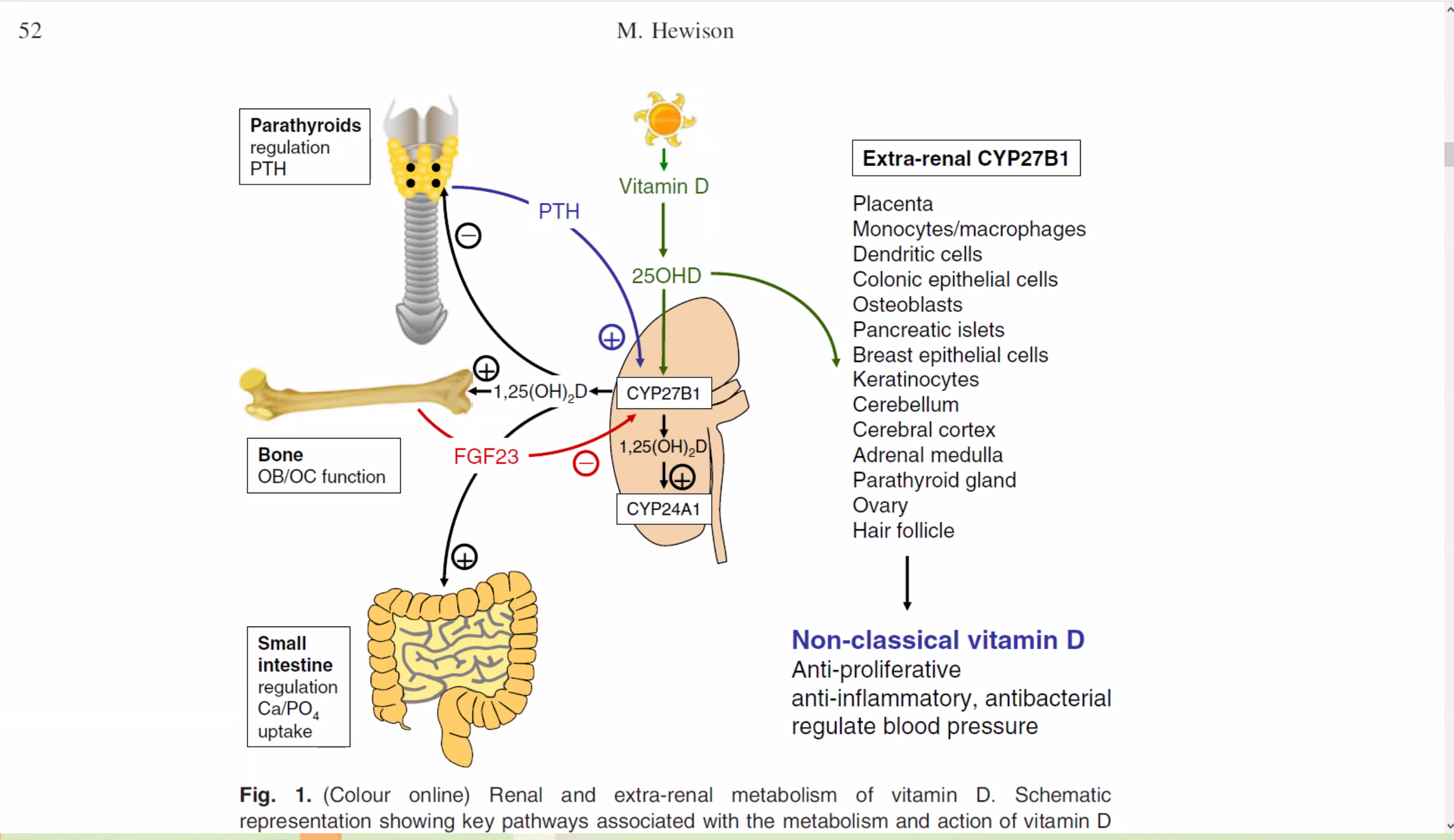
Crucial non-skeletal functions of Vitamin D

Metabolism of 25-Hydroxyvitamin D to 1,25-Dihydroxyvitamin D for Nonskeletal Functions.
“Brain, prostate, breast, and colon tissues, among others, as well as immune cells have a vitamin D receptor and respond to 1,25-dihydroxyvitamin D, the active form of vitamin D…Directly or indirectly, 1,25-dihydroxyvitamin D controls more than 200 genes, including genes responsible for the regulation of cellular proliferation, differentiation, apoptosis, and angiogenesis. It decreases cellular proliferation of both normal cells and cancer cells and induces their terminal differentiation.”
“1,25-Dihydroxyvitamin D is also a potent immunomodulator…1,25-dihydroxyvitamin D3 inhibits renin synthesis,increases insulin production, and increases myocardial contractility…Serum 25-hydroxyvitamin D is not only a predictor of bone health but is also an independent predictor of risk for cancer and other chronic diseases.”
Besides osteoporosis, fracture, loss of muscle strength and falls, he goes on to explain how cancer, autoimmune diseases, osteoarthritis, diabetes, schizophrenia, depression, lung function and wheezing illnesses are consequences of inadequate vitamin D.
It is now generally accepted that vitamin D deficiency is a worldwide health problem that affects not only musculoskeletal health but also a wide range of acute and chronic diseases.
The authors of Vitamin D for Health: A Global Perspective published in Mayo Clinic Proceedings state:
“Vitamin D deficiency has been recognized as a pandemic with a myriad of health consequences.1,2 Low vitamin D status has been associated with an increased risk of type 1 diabetes mellitus, cardiovascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy, and even frailty.1-4 Low prenatal and neonatal vitamin D status may also increase susceptibility to schizophrenia, type 1 diabetes, and multiple sclerosis (MS) in later life via specific target organ effects, including the immune system, or through epigenetic modification.5”
They highlight these points:
Vitamin D deficiency is a common underdiagnosed condition.
Recent evidence from hundreds of studies suggests that vitamin D is important for reducing the risk of type 1 diabetes mellitus, cardiovascular disease, certain cancers, cognitive decline, depression, pregnancy complications, autoimmunity, allergy, and even frailty.
The blood level of 25(OH)D is the best method to determine vitamin D status.
Vitamin D deficiency during pregnancy may influence fetal “imprinting” that may affect chronic disease susceptibility soon after birth as well as later in life.
An effective strategy to prevent vitamin D deficiency and insufficiency is to obtain some sensible sun exposure, ingest foods that contain vitamin D, and take a vitamin D supplement.
“As a consequence of this new perspective on adequate vitamin D levels, it has been suggested that sub-optimal vitamin D status, vitamin D insufficiency, is much more common than previously thought.
The noted vitamin D researcher Martin Hewison states in ‘Vitamin D and immune function: an overview’:
“Collectively these observations suggest that vitamin D is a key factor linking innate and adaptive immunity, and both of these functions may be compromised under conditions of vitamin D insufficiency…As such, vitamin D has the potential to influence a wide range of immune disorders, notably infectious and autoimmune diseases. At a clinical level, associated studies have expanded functional data to show that vitamin D insufficiency is linked to several common immune health problems.”
The many ‘non-classical’ effects of vitamin D function can be degraded due to various impediments.
10 years later the same authority, in a paper entitled ‘The vitamin D deficiency pandemic’, states:
“Vitamin D deficiency and insufficiency is a global health issue that afflicts more than one billion children and adults worldwide.
“The consequences of vitamin D deficiency cannot be under estimated. There has been an association of vitamin D deficiency with a myriad of acute and chronic illnesses including preeclampsia, childhood dental caries, periodontitis, autoimmune disorders, infectious diseases, cardiovascular disease, deadly cancers, type 2 diabetes and neurological disorders.”
Impediments to Vitamin D function
There are numerous factors that can interfere with vitamin D absorption, release to tissues, and tissue response They result in a functional deficiency that can require higher serum levels to accomplish the same effect result for which lower levels would suffice in an individual without those impediments. Very common ones include:
Diminished receptivity of the VDR (vitamin D receptor)* by pathogens, including the herpes family of viruses, especially EBV (Epstein-Barr Virus), HepB, Aspergillus, etc.; or genetics.
Inhibited VDR function* due to high levels of ROS (reactive oxygen species), very common. This includes hydrogen peroxide (H2O2) production and high glucose levels.
Insufficient production of Interferon-gamma (IFN-g) by immune cells due to immune system polarization impairs activation of 25-OH Vitamin D to the active 1,25-OH Vitamin D. This is commonly due to Th2 dominance with increased production of IL-4.
High Vitamin D Binding Protein (VDBP) binding affinity, resulting in poor release of vitamin D from the serum to tissues.
Iron or magnesium insufficiency impairs the vitamin D conversion enzyme.
Selective retention of vitamin D in adipose tissue in overweight conditions.
Acquired vitamin D resistance is also described in settings such as infection, cancer, and autoimmune disease, where epigenetic and transcriptional changes in the RXR/VDR nuclear receptor heterodimer complex blunt signaling even when vitamin D levels are adequate.
Intestinal fat malabsorption (vitamin D is fat soluble).
*The PTH (parathyroid hormone) should be in the bottom third of the reference range as an indication of good VDR function.

VDR function and inhibition - Cogence Immunology
Vitamin D Toxicity - How much is too much?
As noted above, providers untrained in vitamin D biology can be misled by the standard reference ranges and dosages often required to accomplish vitamin D functional sufficiency. But where to draw the line? When do serum levels of vitamin D (25-OH Vitamin D) actually risk toxicity?
“The evidence is clear that vitamin D toxicity is one of the rarest medical conditions and is typically due to intentional or inadvertent intake of extremely high doses of vitamin D (usually in the range of >50,000-100,000 IU/day for months to years).”12
In an editorial published in Mayo Clinic Proceedings entitled ‘Vitamin D Is Not as Toxic as Was Once Thought: A Historical and an Up-to-Date Perspective’, the author notes:
“With all the publicity surrounding the health benefits of vitamin D, health care professionals have begun to routinely measure serum 25(OH)D levels and treat their patients with vitamin D. However, the Institute of Medicine raised concerns about widespread vitamin D supplementation potentially causing harm. Of note, it found that vitamin D deficiency was associated with increased risk for mortality. However, it cautioned that when blood levels of 25(OH)D were more than 30 ng/mL, there was the potential for increased risk for mortality, and it cautioned that blood levels of 25(OH)D should not be more than 50 ng/mL.”
“The current report of Dudenkov et all sheds light on the appropriateness of the Institute of Medicine recommendation. Dudenkov et all evaluated more than 20,000 25(OH)D measurements performed at Mayo Clinic from 2002 to 2011 and related blood levels of 25(OH)D of more than 50 ng/mL with potential vitamin D toxicity (as determined by the presence of hypercalcemia). They observed that from 2002 to 2011, there was a more than 20-fold increase in the number of individuals with serum 25(OH)D levels of more than 50 ng/mL; however, elevated serum 25(OH)D levels were not statistically significantly related to serum calcium values.”
“This discovery of Dudenkov et al1is logical because the body tightly controls the conversion of 25(OH)D to 1,25-dihydroxyvitamin D, which is responsible for regulating calcium metabolism by enhancing intestinal calcium absorption and mobilizing calcium from the skeleton…Dudenkov et al also found that only 1 person with a serum 25(OH)D level of 364 ng/mL had evidence of clinical toxicity, that is, hypercalcemia. For comparison, the Endocrine Society’s practice guidelines on vitamin D state that vitamin D intoxication is usually not observed until serum 25(OH)D levels are more than 150 ng/mL.”
“Vitamin D intoxication associated with hypercalcemia, hyperphosphatemia, and suppressed parathyroid hormone level is typically seen in patients who are receiving massive doses of vitamin D in the range of 50,000 to 1 million IU/d for several months to years. Ekwaru et al16recently reported on more than 17,000 healthy adult volunteers participating in a preventative health program and taking varying doses of vitamin D up to 20,000 IU/d. These patients did not demonstrate any toxicity…”
“There remains concern, however, that increasing vitamin D intake even by 400 IU/d increases the risk for kidney stones, especially in patients with a history of kidney stones.10 Despite this concern, there is no credible scientific literature suggesting that such vitamin D intake increases the risk for kidney stones.12,15 Similarly, data are weak regarding the association between vitamin D intake and cardiovascular calcifications.12 To the contrary, current evidence suggests that improvement in vitamin D status reduces the risk for hypertension, stroke, and myocardial infarction.12”
“The evidence is clear that vitamin D toxicity is one of the rarest medical conditions and is typically due to intentional or inadvertent intake of extremely high doses of vitamin D (usually in the range of >50,000-100,000 IU/d for months to years)…
In the very rare occurrence of toxicity (due to granulomatous disorders including sarcoidosis, William syndrome, some lymphomas, and the rare genetic disorder of the absence of the 25-hydroxyvitamin D-24-hydroxylase)…
“Simply reducing the calcium intake, wearing sun protection to prevent vitamin D production, and eliminating all vitamin D from dietary sources will result in a gradual decrease in serum 25(OH)D levels, with no significant sequelae from the toxicity.”2,12

Disassociation of Vitamin D’s Calcemic Activity and Non-calcemic Genomic Activity and Individual Responsiveness: A Randomized Controlled Double-Blind Clinical Trial
This insightful research further raises understanding of the benefits of higher doses of Vitamin D.
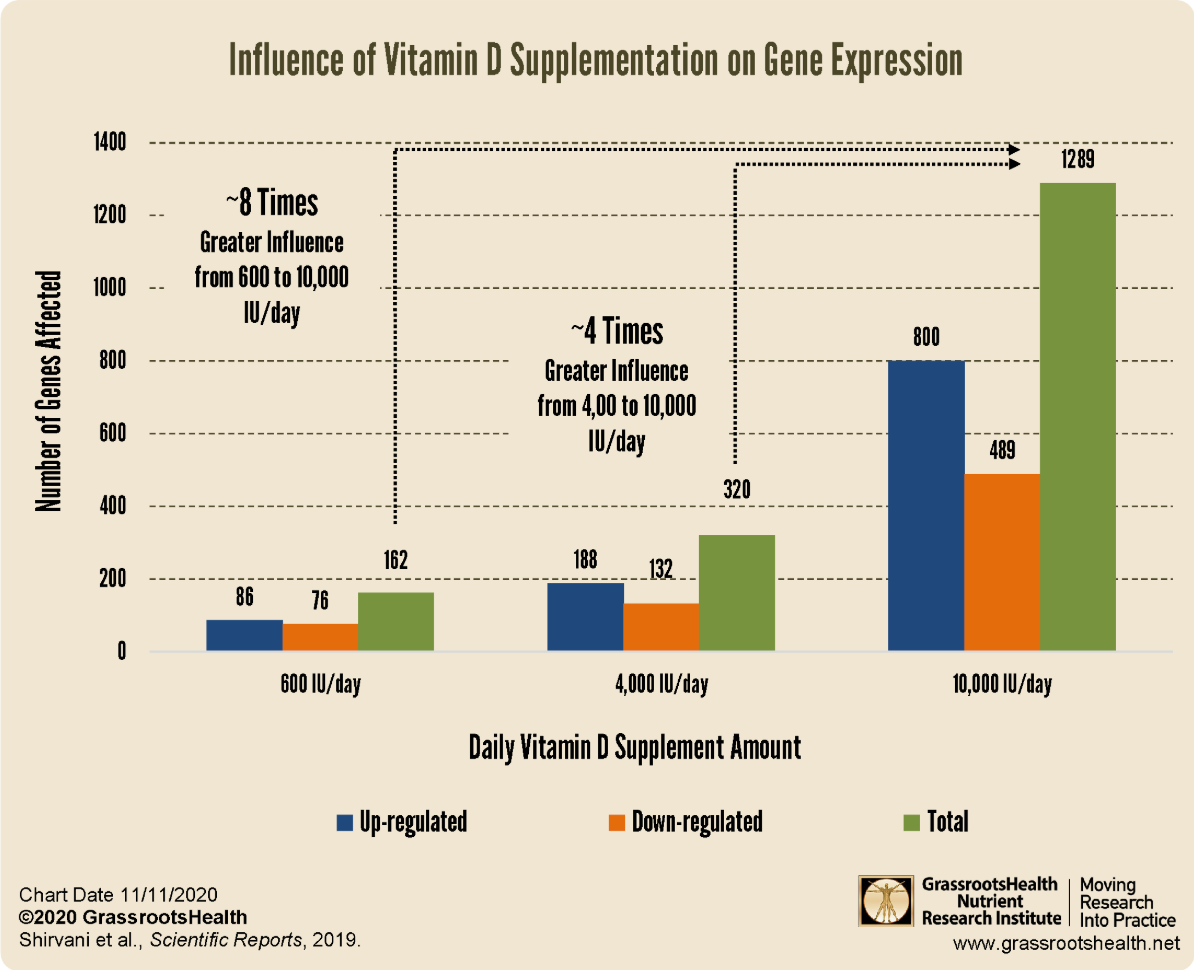
In a fascinating and important research published in Nature Scientific Reports, the authors show evidence that the genetic response to vitamin D continues to improve as serum levels increase beyond that required for sufficiency as indicated by PTH (parathyroid hormone) levels. The authors state:
“The aims of this randomized controlled double-blind clinical trial were to assess the impact of vitamin D supplementation on calcium metabolism and non-calcemic broad gene expression by relating them to the individual’s responsiveness to varying doses of vitamin D3. Thirty healthy adults were randomized to receive 600, 4,000 or 10,000 IU/d of vitamin D3 for 6 months. Circulating parathyroid hormone (PTH), 25(OH)D, calcium and peripheral white blood cells broad gene expression were evaluated. We observed a dose-dependent increase in 25(OH)D concentrations, decreased PTH and no change in serum calcium. A plateau in PTH levels was achieved at 16 weeks in the 4000 and 10,000 IU/d groups.”
HOWEVER:
“There was a dose-dependent 25(OH)D alteration in broad gene expression with 162, 320 and 1289 genes up- or down-regulated in their white blood cells, respectively. Our results clearly indicated that there is an individual’s responsiveness on broad gene expression to varying doses of vitamin D3. Vitamin D3 supplementation at 10,000 IU/d produced genomic alterations several fold higher than 4,000 IU/d even without further changes in PTH levels. Our findings may help explain why there are some inconsistency in the results of different vitamin D’s clinical trials.”
In comparison to the standard recommendations…
“Studies evaluating supplementation with vitamin D up to 2000 IU/d with an average of 5 years of follow-up did not find benefit for reducing risk for cardiovascular disease or cancer13. In the Vitamin D and Omega-3 Trial (VITAL)13, a large primary-prevention trial, supplementation with vitamin D3 (at a dose of 2,000 IU/d) did not show any significant association with lower occurrence of cardiovascular events or invasive cancer than placebo13. Despite that vitamin D supplementation did not associate with a lower occurrence of total deaths from cancer than placebo, yet found that mortality due to cancer was significantly lower with vitamin D supplementation13. Patients’ quality of life in hospital was improved after supplementation with vitamin D3 at 10,000 IU/d over 6 months and improved hormonal factors b-type natriuretic peptide (BNP) and PTH as well as inflammation14. These findings suggest possible health benefits of doses of vitamin D above the RDA.”
In regard to the influence of vitamin D supplementation on genome-wide expression, which had remained largely unexplored in vivo, particularly with respect to dose:
“Pathway and functional analysis of the target genes indicated that vitamin D supplementation may be connected with some pathways related to epigenetic modification, immune system and response to stress8. Many of these activities of vitamin D have been hypothesized to play roles in disease susceptibility including autoimmune disease and cancer8,12. The current clinical trial was designed to evaluate the responsiveness of different doses of vitamin D supplementation (600 IU/d, 4,000 IU/d and 10,000 IU/d) on serum calcium, PTH and broad gene expression in white blood cells.”
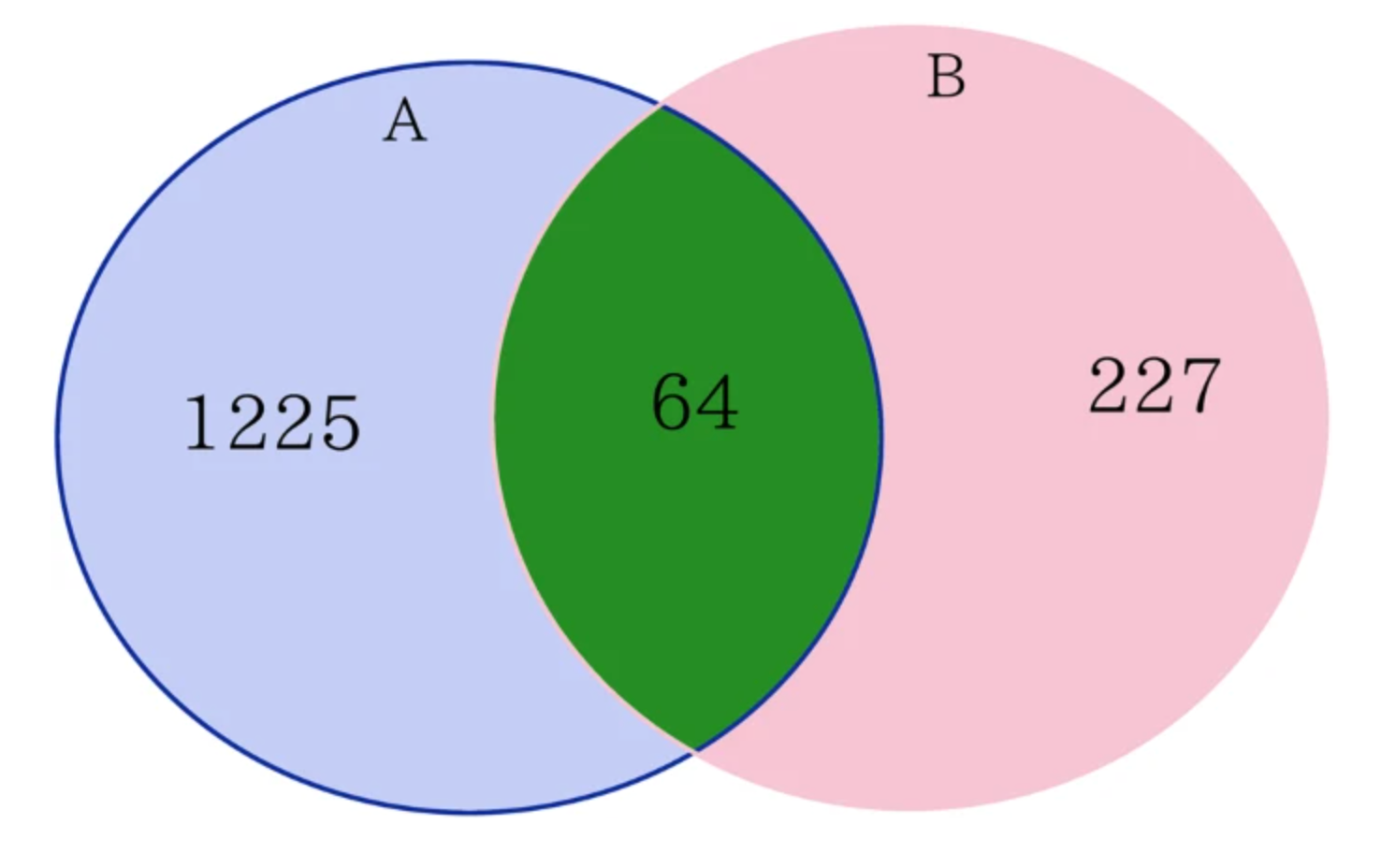
Venn diagram for comparing the number of affected genes between current study and our previous study8. (A) Differential expression analysis identified 1289 DEGs (differentially expressed genes) after 24 wks vitamin D3 supplementation (10,000 IUs/d). (B) Differential expression analysis identified 291 DEGs after 8 wks vitamin D3 supplementation (400 or 2,000 IUs/d).
The authors further state:
“There continues to be controversy as to whether reaching blood concentrations of 25OH)D above 30ng/mL would have any additional health benefits3,12. Our results demonstrated that PTH plateaued when 25(OH)D ≥ 30 ng/mL (75 nmol/L) and confirms previous observations that serum concentrations of PTH continued to decrease and reach a plateau when circulating levels of 25(OH)D > 30 ng/mL24,25,26. The effect of increasing vitamin D3 from 4,000 IU/d to 10,000 IU/d had no significant additional effect on the PTH levels (Fig. 2). However, the gene expression analysis demonstrated a dose dependent effect. Even for subjects who took 600 IU/d of vitamin D3 for 24 weeks, a dose that had little effect on PTH levels, this dose significantly affected the expression of more than 100 genes. In comparison, the groups who received vitamin D3 supplement 4,000 and 10,000 IU/d for 24 weeks had a similar effect on lowering the blood levels of PTH, but the group who received 10,000 IU/d had 4-fold greater effect on gene expression, influencing ~1,200 genes compared to the group who took 4,000 IU/d (about 300 genes). These results indicated that even a small increase in vitamin D3 intake of 600 IU/d for 24 weeks, a dose that did not alter the PTH levels, exerted significant genomic effects. Therefore, randomized controlled trials that include a “placebo” group receiving the RDA of 600 IU/d are confounded by unanticipated changes in gene expression. Our findings showed that there was a dissociation between the calcemic and non-calcemic biologic actions of vitamin D3, especially on functions involved in immune activity.”
“These results may help explain the disparity of conclusions regarding the studies that have evaluated the impact of supplementation with vitamin D3 on serum 25(OH)D improvement and clinical outcomes. An individuals response to vitamin D3 is related to the individual’s ability to convert vitamin D to its active metabolite and 1,25(OH)2D’s interaction with its receptor and response elements8,27,28.”
Their conclusion has great clinical importance:
“This research program emphasizes the importance of personalized medicine. Vitamin D supplementation at 10,000 IU/d for 6 months was safe, had optimally regulated PTH levels and a pronounced effect on genetic expression of more than 1,200 genes. Furthermore, broad gene expression may predict individual responsiveness to vitamin D3 supplementation.”
How high can you go without toxicity?
Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”
The effect of extremely high doses of Vitamin D3 in the treatment of autoimmune diseases.
In this dramatic research paper published in the journal Nutrients, the authors report on their investigation of the safety and tolerability of the Coimbra Protocol that has, under careful medical management, applied 35,000 IU up to 150,000 IU of vitamin D per day over extended periods of time. It is also an excellent review of key points of vitamin D function and evaluation of the effectiveness of supplementation in case management.
Providers should be informed about three principles highlighted by this study: that there is significant individual variation in response to vitamin D due to genetic and other factors; that some individuals require very high doses for therapeutic effectiveness; that PTH (parathyroid hormone) levels in response to supplementation are a gauge of VDR (vitamin D receptor) response; and that, professionally managed, even ultra-high therapeutic doses have been given without toxic effects.
The authors note:
“The worldwide increase in patients with autoimmune diseases during the last decades [1] has led to a significant challenge to our health systems, both therapeutically and economically [2,3]. The etiology of autoimmune diseases is multifactorial, involving a combination of genetic and environmental factors. Numerous different mechanisms, including exposure to environmental pollution and toxins, the complex mechanisms of lifestyle factors (e.g., “Western diet”, smoking and alcohol consumption, psychosocial stress), infections, and intestinal dysbiosis, are attributed to initiate complex pathogenetic cascades leading to systemic or organ-specific autoimmune conditions” [4,5].
“Independent of a broad spectrum of therapeutic strategies for the many different autoimmune diseases that we can offer our patients today, an integrative approach to treatment should be our goal. Although it is questionable whether the pathogenetic complexity of all autoimmune diseases can be focused on one central or specific factor, there is accumulating evidence for an important regulatory role of the biologically active hormone/Vitamin D (1,25-dihydroxyvitamin D3;1,25(OH)2D3) in this context [6].”
Role in the immune system
“Vitamin D has a complex role in the immune system, regulating both innate and adaptive immunity and resulting in the inhibition of inflammation and the enhancement of defense mechanisms [7,8]. Mediated by the vitamin D receptor (VDR), 1,25(OH)2D3 can influence immune function as well as the differentiation and growth of many cell types in addition to its well described central role in bone metabolism [7,9,10].”
“We and others have demonstrated an association of serum levels of 25(OH)D and numerous chronic diseases, including inflammatory skin diseases (e.g., psoriasis and atopic dermatitis), autoimmune reactions (e.g., rheumatoid arthritis, multiple sclerosis, and vitiligo), inflammatory conditions as well as cardiovascular diseases, diabetes mellitus, metabolic syndrome, certain malignant tumors (e.g., breast, colon, and prostate), diseases of the central nervous system brain (e.g., schizophrenia, Alzheimer’s disease, and depression), and infections (upper respiratory tract, tuberculosis, and COVID-19) [9,11,12,13]. Vitamin D status is also considered to be of high importance for longevity [14,15].”
The Coimbra Protocol
The Coimbra Protocol uses ultra-high dosages of vitamin D. It proved to be very successful for the autoimmune conditions treated. Of particular interest here is that even these huge doses did not result in toxicity for the study subjects.
“Coimbra and co-workers, after two decades of clinical experience, state that the therapeutic approach of the protocol relies on doses of vitamin D that range from 40,000 IU to 300,000 IU per day [17,18]. The conventional starting dose in multiple sclerosis, for example, is approximately 1.000 IU vitamin D3 per kg body weight [19].”
These protocol has also been used in Germany too:
“In Germany, this therapeutic protocol for autoimmune patients has been used since 2016 [20]. Underlying the CP is the hypothesis of the non-hereditary, but acquired form of vitamin D resistance and insufficient biological activity of 1,25(OH)2D3, which both may be overcome by high doses of vitamin D3, compensating the resistance. Lemke et al. have recently elegantly elaborated the background of an acquired vitamin D resistance as a possible cause of autoimmune diseases and could confirm this hypothesis of the malfunction of the vitamin D metabolism underlying the efficacy of high-dose vitamin D CP [19].”
“According to their proof of concept, single nucleotide polymorphisms (SNPs) within the genes of the vitamin D system (e.g., in activating enzymes, serum transport, and VDR) cause individual vitamin D resistance and reduced vitamin D responsiveness.PTH [parathyroid hormone] serum levels serve as valuable biomarker for vitamin D3 dosing and its effect on altering calcium metabolism [19].”
Moreover…
“To date—apart from the high-dose vitamin D protocol—no other causal treatment for correcting a blockade of the VDR is known.”
[These ultra-high doses were closely clinically managed, accompanied by good hydration (2.5L water per day), a strict low calcium diet, no calcium supplements, and regular laboratory evaluations.]
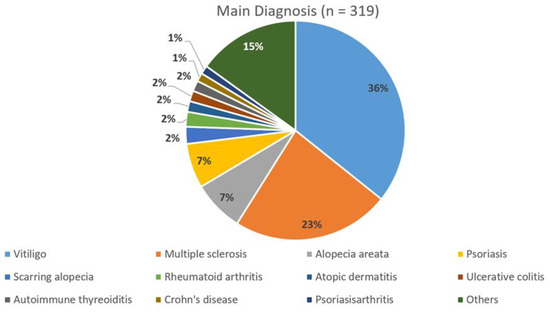
Autoimmune diagnoses in this study of the Coimbra Protocol
The doses of vitamin D were ultra high:
“Vitamin D3 was taken orally according to dose recommendations of CP [19] at 1000 IU/kg body weight for MS and 300–1000 IU/kg body weight for the majority of other autoimmune diseases.The maximum dose in our population was 150,000 IU per day (Table 1), mean dosage for all patients was 35,291 ± 21,791 (SD) IU per day, whereas mean dosage for patients with MS was significantly higher than for patients without MS (52,955 ± 25,791 IU per day vs. 29,683 ± 16,861 IU per day, p < 0.0001, Table 1).”
Importantly…
“The onset of clinical symptoms suggestive of hypercalcemia [the first sign of vitamin D toxicity] (increased thirst, constipation, nausea, and vomiting) was not reported at any time…When we then compared the parameters for single patients at baseline with their average follow-up values, we could not detect renal impairment or any clinically relevant changes in the serum calcium and 24 h urinary excretion (Figure 4)…This further confirms the safety of high doses of orally applied vitamin D3, as increases in dosages are—under appropriate doctoral supervision—only moderately correlated with the subsequent serum and urinary calcium measurements.”
The authors conclude:
“In the pilot study of Coimbra’s group published in 2013 [16], assessing the effect of the prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis, nine patients with psoriasis and sixteen patients with vitiligo received vitamin D3 35,000 IU once daily for six months in association with a consequent low-calcium diet (avoiding dairy products and calcium-enriched foods, such as oat, rice or soya “milk”) and reliable hydration (minimum 2.5 L daily). In their study, serum creatinine and calcium (total and ionized) did not change and urinary calcium excretion increased within the normal range [16].”
“To our knowledge, we in this paper demonstrate for the first time for a broad spectrum of autoimmune diseases in over 300 patients with a treatment period of more than 3.5 years that high doses of orally applied vitamin D3 up to 1000 IU per kg bodyweight are safe in terms of calcium metabolism and renal function, when strict recommendations for diet and fluid intake are followed, up to a treatment period of 3.5 years.”
“For many years, we have been following clinically the recommendation of 25(OH)D ranging between 40 and 60 ng/mL being considered to be “optimal” (preferred range) for healthy people [9,58,59,60]. However, for autoimmune and inflammatory diseases, we have little knowledge about the variations of vitamin D metabolism and recognition, such as VDR polymorphisms, vitamin D binding protein polymorphisms, extrarenal 1 alpha hydroxylase activity, and micro RNAs[61].”
“With respect to our population, the mean daily dose of 35,000 IU Vitamin D3 is far higher than usual recommendations [57] and should be a contribution to the debate on the disparity of conclusions on what an “optimal” serum concentration of 25(OH)D is and how much supplementation is required to achieve a sufficient clinical response without long-term side effects.”
“Instead of solely focusing on 25(OH)D serum levels, different groups have recently elegantly worked out that, due to epigenetic and genetic differences, the individual immune responsiveness to vitamin D3 is rather complex [19,57,62,63]. Among other factors, this depends on the individual ability to convert vitamin D to its active metabolite 1,25(OH)2D and the interaction with VDR and the response elements [62,63,64]. Recently, it was shown that there is a dissociation between the calcemic and non-calcemic biologic actions of vitamin D3, especially on functions involved in immune activity [57].
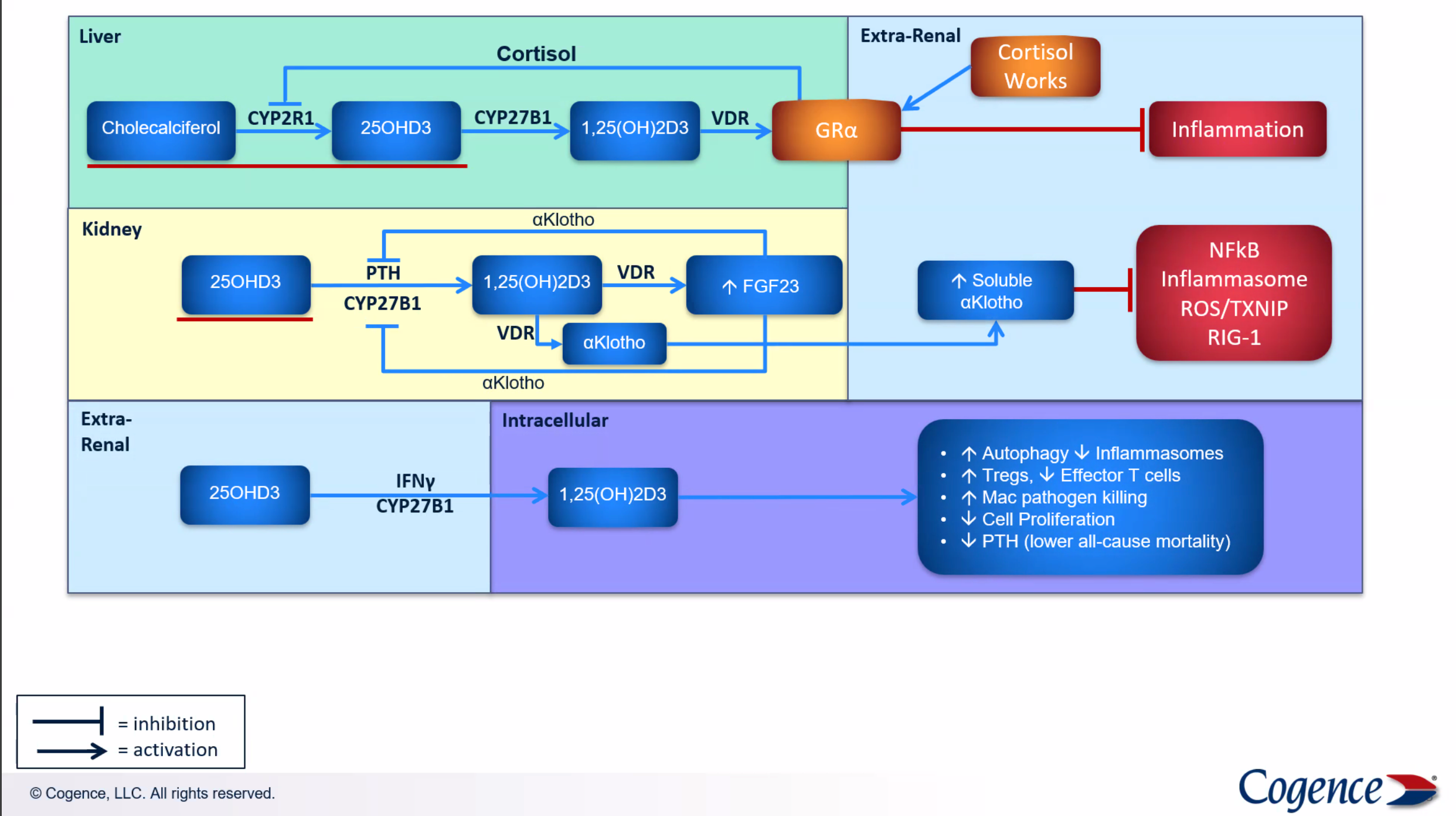
Vitamin D conversion and regulation of inflammation - Cogence Immunology
“Against this background, the suppression of PTH should be rather favored as a proxy for optimal vitamin D status as well as vitamin D3 treatment [65].”
“As previously shown, the genetic polymorphism of CYP27B1 associated with autoimmunity [66,67] causes a relative resistance to vitamin D requiring a higher level of circulating 25(OH)D3 to achieve biologically active 1,25(OH)2D3, resulting in normalized immune functions [16]. In order to achieve a physiologic rate of product formation in polymorphic enzyme variants, a higher Km (decreased affinity for substrate) and/or a lower Vmax require supra-physiologic concentrations of the substrate [16].”
In patients with a combination of polymorphisms within different sections of vitamin D metabolism, this effect is potentiated. Supra-physiologic doses as applied according to CP may compensate for this genetic-related status of relative vitamin D resistance establishing tolerance to auto-antigens and may with respect to our safety data also increase tolerability in patients with autoimmune disorders [16]. This might explain the far lower PTH plateau in our patients in comparison with healthy subjects studied by Shirvani and co-workers [57].
“According to Lemke et al. and the hypothesis of Cicero Coimbra of an acquired vitamin D resistance in autoimmune diseases [19], PTH concentrations could be used as a hallmark for individual adaption of oral vitamin D3 dosages. For an optimal physiological response of 1,25(OH)2D3, a low PTH plateau should reached and maintained within the lower third of the reference range [19]. With respect to our own experiences during the last four years, the degree of inflammation in autoimmune processes seem to influence the need to further decrease the PTH level by higher daily doses of vitamin D3.”
“A seven-year experience of McCullough et al. with oral vitamin D3 up to 50,000 IU per day did not reveal a linear or exponential relationship between vitamin D and calcium blood levels [68]. They did not observe cases of vitamin D3 induced hypercalcemia or any adverse events attributable to vitamin D3 supplementation in any patient.”
“With our current detailed knowledge about vitamin D metabolism, central cofactors (e.g., magnesium [69]), the influence of SNPs according to (epi)genetic studies [39], and worldwide experience of several thousands of patients treated with the CP from 2012 onwards with daily doses up to 340,000 IU [70], we are able to develop an individualized vitamin D3 treatment for autoimmune patients by the careful planning and determination of reliable mechanisms for regular laboratory controls. Based on our findings, hypercalcemia does not appear to be a first line risk of high-dose vitamin D3 therapy.”
“Despite our evidence that high-dose vitamin D3 application according to CP is generally well tolerated without signs for long term toxicity, this therapeutic approach of vitamin D3 supplementation should be embedded in a holistic treatment package. Against this background, fascinating new findings from gut microbiome research demonstrated variations in the vitamin D receptor also influence the large functional network of gut microbiota [81].”
“In summary, to our knowledge, our work provides the first long-term documentation of selected critical laboratory parameters during the application of the CP using a high-dose oral vitamin D3 in a broad spectrum of different autoimmune diseases, demonstrating that this procedure is well tolerated with respect to renal function and calcium metabolism. In terms of individualized treatment, we suggest to further use serum levels of PTH as biomarker for an individual response to vitamin D3, the individual ability to convert vitamin D to the active metabolite, the 1,25(OH)2D’s interaction with its receptor and the response elements and finally the differential supplementation with vitamin D3. In further studies, possible differences of the clinical outcome of CP treatment should be investigated.”
“We strongly recommend that CP is always used in the hands of qualified and experienced physicians and strongly advise against the use of CP by patients themselves based on Internet information.”
New studies are continuously being published
The papers cited in this post offer a brief sampling of the extensive literature on vitamin D supplementation. New ones are frequently appearing. Here are just a few examples published in the last few weeks.
Vitamin D promotes immune tolerance to gut microbiota in patients with IBD
“Loss of immune tolerance to the gut microbiome plays a pathogenic role in inflammatory bowel disease (IBD)…Vitamin D treatment associates with decreased disease activity and inflammatory markers and increased IgA-bound and decreased IgG-bound gut microbiota…Our results demonstrate that vitamin D promotes immune tolerance to gut microbiota in patients with IBD.”

ApaI genotyping [of the VDR may identify adults with prediabetes who experience benefits from high-dose vitamin D3 supplementation to lower their risk of developing diabetes.”

Association of Circulating Vitamin D in Midlife With Increased Tau-PET Burden in Dementia-Free Adults
“In a group of dementia-free individuals, higher serum 25(OH)D at early midlife was associated with lower tau deposition on brain-PET a mean of 16 years later. Low vitamin D in midlife may represent a potentially modifiable target to mitigate the risk of neuroimaging signs of preclinical dementia.”